

The ‘Saving babies’ lives' care bundle identified effective fetal monitoring during labour as one of four key areas of care to reduce the number of stillbirths and early neonatal deaths in the UK (NHS England, 2016). Intrapartum cardiotocograph (CTG) interpretation is a key midwifery skill in which midwives must prove competency prior to registration and annually thereafter if caring for women in a birth setting (NHS England, 2016; Nursing and Midwifery Council [NMC], 2019). However, the most recent ‘Each baby counts’ report (Royal College of Obstetricians and Gynaecologists, 2019), which reviewed the care of women whose babies died or were severely disabled as a results of incidents occurring during term labour in 2017, found that CTG issues were a critical contributory factor in the care of 59% of cases in which different care may have affected outcomes. Similarly, the most recent perinatal confidential enquiry noted that ‘there were errors in the method, interpretation, escalation and response to fetal monitoring’ which were a contributing factor in several intrapartum deaths (Draper et al, 2017).
CTG interpretation has been described as a ‘high-level skill [which] is susceptible to variation in judgment between clinicians and by the same clinician over time’ (NHS England, 2016). Therefore, it is crucial that midwives are able to confidently support student midwives to develop this skill. While the ‘Future midwife’ standards state that principles and methods of teaching should be included in the undergraduate midwifery curricula, at present, that is rarely the case and, as a result, midwives are not always able to convey their knowledge and skills to students in a clear, effective way (Sweet et al, 2017; NMC, 2019). Knowledge of teaching and learning theories, and of learning styles, can enable midwives to maximise clinical learning while also consolidating their own practice and knowledge (Rance and Sweet, 2016). This article uses a case study to examine how practice assessors can best teach students to safely and accurately undertake and interpret CTG monitoring according to national guidelines.
In this case study, CTG interpretation was taught to a third-year student midwife, Aaliyah (pseudonym used to maintain confidentiality), by hourly reviews of a live CTG over the course of a single 12-hour night shift on labour ward. Aaliyah had identified CTG interpretation as a learning need during her initial interview with me, her practice assessor.
Create a psychologically safe learning environment
The humanistic theory of learning incorporates not only knowledge but personal growth (Gopee, 2015). Maslow (Bailey-McHale and Hart, 2013) proposed that learning, or self-actualisation is an intrinsic psychological need. In his renowned ‘Hierarchy of needs’, Maslow theorised that in order for self-actualisation to take place, basic physiological and safety needs must be met in addition to psychological needs such as respect, confidence and a sense of belonging. As a consequence of this, in a clinical environment where a student feels criticised or ashamed for lack of knowledge, learning will be negatively impacted. Aaliyah confided that she had found it difficult to maintain a good working relationship with her previous labour ward mentor who she felt was overly critical of her knowledge and abilities. In her opinion, she felt ‘on edge’ when working with this mentor and that her learning was affected.
The theory was further advanced by Rogers (Kilgallon and Thompson, 2012) who, dismayed by what he perceived as an overemphasis on cognitive processes in education, argued that the true goal of education is personal growth and development. Rogers advocated for student-centred learning and recommended that the teacher act as facilitator, focusing on establishing a genuine relationship with the learner and valuing each student as an individual. However, while there are undoubtedly benefits to creating a relationship of mutual respect, it could be argued that the characteristics of unconditionally trusting and accepting students conflicts with the mentor's responsibility to assess and potentially fail students (Bailey-McHale and Hart, 2013).
Humanistic learning theories are founded on the premise that students will learn best when learning is self-directed. Aaliyah reported that she did not enjoy studying physiology and, as a result, was weak in this area. However, Pinas and Chandrahandran (2016) propose that an in-depth understanding of the physiology underpinning fetal heart rate changes is necessary to correctly interpret CTGs. Therefore, the humanistic approach is limited and can be seen to have flaws as adhering strictly to this style may result in gaps in knowledge. Nevertheless, the principles of humanistic teaching provide a good basis for enjoyable and effective teaching. Sharp et al (2006) adapted Maslow's ‘Hierarchy of needs’ for mentors and further adaptations were made by Stuart et al (2013) as shown in Figure 1. These ideas were incorporated in the teaching of Aaliyah: for example, ensuring her comfort needs were met, addressing her concerns and introducing her to the team and labouring woman and her family in order to foster Aaliyah's sense of belonging.
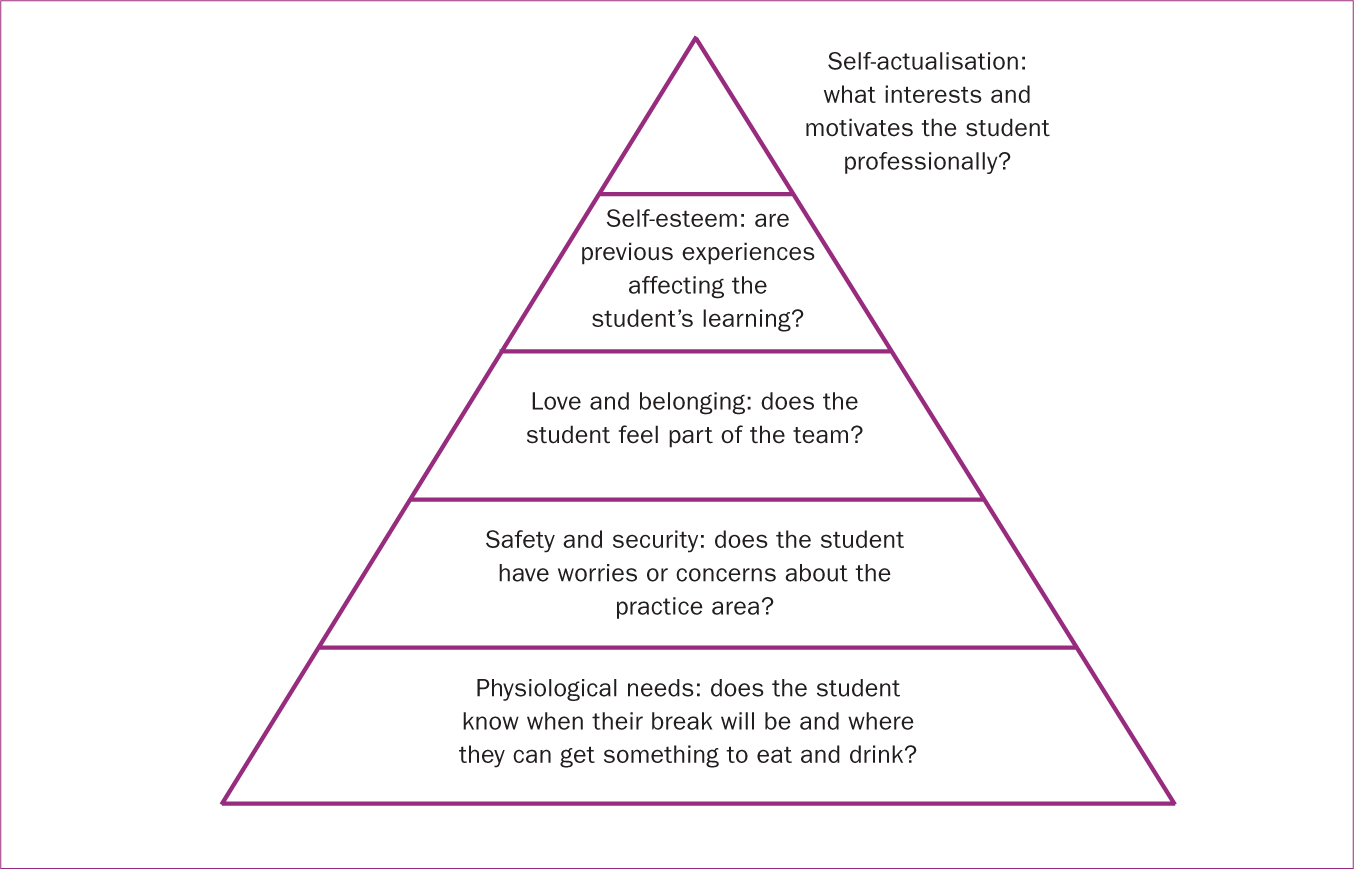 Figure 1. Maslow's ‘Hierarchy of needs’,
Figure 1. Maslow's ‘Hierarchy of needs’,
Develop higher order thinking skills
The cognitive theory of learning focuses on the process of learning and assumes that learning is not imposed by the teacher but is instead an active process whereby the learner adds new information to existing knowledge, skills and experiences. Bruner (Walsh, 2010) proposed that teaching should be easy to understand, logically sequenced and made interesting to the student-for example, use of a problem-solving model rather than lecturing dry theory. Bloom's taxonomy of learning (Gopee, 2015) identifies the cognitive processes involved in learning and arranges them in hierarchical order, from lower order thinking skills – such as knowledge and comprehension – to higher order thinking skills, such as evaluation.
Critics of the taxonomy argue that learning does not always take place in a sequential, hierarchical manner and that cognitive learning theories ignore the individuality of the student and the environment in which they learn (Gopee, 2015). However, the concepts of cumulative learning – confidently grasping fundamentals of knowledge before applying that knowledge to problem-solving – and actively applying new knowledge to existing information is useful as a teaching tool and was used in this instance. Table 1 shows how I adapted Bloom's taxonomy to this activity so that Aaliyah's current ability could be determined and a structured approach to teaching CTG interpretation used.
Table 1. Bloom's taxonomy of learning
| Discuss the evidence for and against electronic fetal monitoring | Evaluation |
| Hypothesise solutions for an abnormal cardiotocograph (CTG) | Synthesis |
| Infer possible causes for an abnormal CTG | Analysis |
| Identify abnormal CTG features | Application |
| Teach the basic features to a more junior student | Comprehension |
| Name the four basic features of CTG | Knowledge |
Adapted by the author to apply to CTG teaching (Bailey-McHale and Hart, 2013)
Identify your student's learning style
Honey and Mumford (Walsh, 2010), building on the earlier work of Kolb, propose that individuals tend to have one of four preferred learning styles – classified as activists, reflectors, theorists and pragmatists – and that identifying and adapting to an individual's preferred learning style results in more effective learning. Aaliyah was not aware of Honey and Mumford's work but identified that she preferred to observe skills several times before she felt confident trying them herself; combined with her thoughtful approach and love of study, this suggests Aaliyah would be classified as a ‘reflector’. However, Gopee (2015) notes that students almost invariably draw from a range of different styles. In addition, it has been proposed that encouraging students to adapt to learning styles which may not come naturally to them will ultimately assist the student to benefit from any learning opportunity.
In labour, CTGs are systematically reviewed by the midwife hourly. In order to accommodate Aaliyah's learning style, I led the first review, discussing the decision-making process and conclusions with Aaliyah, and over the next few hours, encouraged her to take increasing leadership so that by the fourth review, she was undertaking the review. Aaliyah's increasing confidence was evident: by the time she had completed three hourly CTG reviews, of her own accord she explained to the woman's partner what features of this CTG provided reassurance of his baby's well-being and at the end of the shift, she ‘handed over’ to the incoming midwife, discussing the key features of the CTG (see Table 2).
Table 2. Honey and Mumford's four learning styles
Activists
|
Theorists
|
Reflectors
|
Pragmatists
|
Adapted from Walsh (2010)
Encourage reflection
Near the end of the shift, I cleared time to allow Aaliyah to reflect on the case and encouraged her to use a reflective journal in her own time in order to assist her development. Ghaye et al (2012) propose that explicit reflective practices improve the confidence and competence of the healthcare worker and, as a result, aid transformation of the practice environment.
Reflection is key to Kolb's theory of experiential learning which stresses the critical role of experience in the learning process (Walsh, 2010). Kolb proposed a spiral of learning in which a person undertakes an experience, reflects upon it, begins to understand the experience and plans how to experiment with it, and then acts upon this new knowledge. Walsh (2010) suggests that the intangible skill of intuition possessed by senior nurses is developed through repetition of this cycle and I believe that reflecting on this case may assist Aaliyah to predict the outcome in a similar future case. I also advised Aaliyah to utilise her new skills to teach junior students CTG interpretation; McLelland and French (2011) found that, despite initial apprehension, peer teaching by student midwives increased confidence not only in the skill being taught but also in clinical teaching itself.
Stuart (2013) notes that feedback is expected and welcomed by students, and that feedback provided as a ‘running commentary’ during clinical activity can be highly motivational as it is current, meaningful and allows theory to be linked to practice. Several feedback models have been developed, including Pendleton's model of feedback; however, the model has been criticised for being rigid and formulaic, and may be most suitable for formal assessments (Stuart, 2013). Instead, informal feedback was provided to Aaliyah throughout the activity, using the key principles for effective feedback identified by Stuart-in particular, fostering a sense of progress, aiming to give specific feedback rather than pleasing but unhelpful statements such as ‘you were brilliant’ and encouraging openness.
Recommendations for best practice
Reflection can also be used by the mentor to improve teaching quality and results by learning from mistakes and repeating achievements. Overall, I feel that the activity was successful. Aaliyah spontaneously fed back that she felt the teaching was useful and thought-provoking, and that she felt her knowledge around CTG interpretation had significantly improved. However, this is a skill which is recognised as complex, with poor inter-observer agreement (Rei et al, 2016), and in order to teach this skill most effectively, Aaliyah and I would benefit from several consecutive shifts together.
Part of a mentor's responsibility is to evaluate and improve the learning environment so I asked for students to be given access to the CTG e-learning programme used by staff. Carbonne and Sabri-Kaci (2016) found that an e-learning programme for cardiotocography analysis effectively improved the performance of maternity staff, although this was not verified by Millde-Luthander et al (2012) who carried out a similar study in Stockholm and found no improvement in competence.
Conclusion
CTG interpretation is a complex skill which student midwives often struggle with. Knowledge and understanding of key learning theories and accommodating the individual learning style of students can help practice assessors to ensure that student midwives get the most benefit from teaching and that teaching is enjoyable for both student and teacher. Teaching skills are included in the ‘Future midwife’ standards but consideration should be given to include teaching skills in continuing professional development for existing midwives who may lack this knowledge.
Key points
- It is critical that midwives can safely and accurately interpret cardiotocographs at the point of registration
- It's therefore crucial that midwives can confidently and competently teach this skill to the student midwives in their care
- Understanding key learning theories enables midwives to provide a solid foundation to help students gain and build knowledge
- Awareness of learning styles empowers midwives to create teaching opportunities which students enjoy and maximises their learning
CPD reflective questions
- Thinking back to your time as a student midwife, did your mentors create a psychologically safe environment for you? How do you aim to do this for the students that you support?
- Bloom's taxonomy of learning is very useful to show the progression from being a novice to achieving competence. How could you apply the taxonomy to another skill, for example: breastfeeding support?
- Which learning style most closely matches yours? Are you an activist who likes to get involved and learns through doing? A reflector who considers what they've seen? A theorist who prefers to understand the theory before taking action? Or a pragmatist who learns by applying ideas in practice?
- Students are encouraged to reflect on interactions with their mentor. With a friend, in your diary, or with your professional midwifery advocate, reflect on a recent encounter with a student. What went well and what could you have improved?